
Webinar: Understanding and Responding to People Who Use Performance and Image Enhancing Drugs
Performance and Image Enhancing Drugs (PIEDs) are the fastest growing drug category reflected in NSP statistics across Australia.
An increasing number of individuals who use steroids and other performance and image enhancing drugs (PIEDS) are accessing Needle and Syringe Programs for injecting equipment.
Watch this online training webinar to learn more about PIEDs and how to effectively support those who use them.

Dr. Tim Piatkowski
Griffith University & QuIVAA
Dr Tim will be discussing: Defining PIEDs, understanding who uses PIEDs and why, exploring how people use PIEDs, recommending appropriate equipment for PIED use, and providing harm reduction info.

Sonya Weith
QuIVAA
Sonya will be discussing women and PIED use.
Questions asked during the live training answered by Dr Tim & Sonya
Where can users get steroids tested? (in specific locations around Australia?)
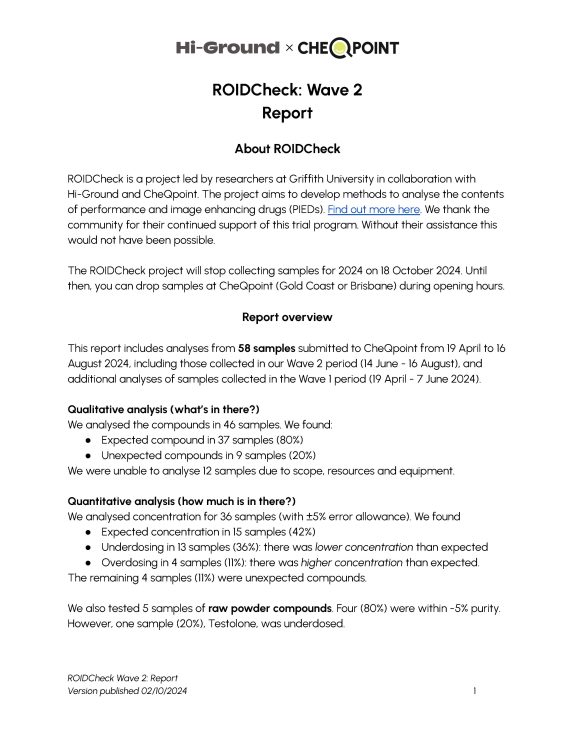
CheQpoint in Brisbane and Gold Coast have been sites of collection for the current steroid checking trial we have underway. Last drop-offs were 18th October 2024 for our Wave 3 analysis.
Results here for waves so far – Steroid Checking Project Results! – hi-ground.org
Watch this space for 2025.
Many side effects of PIEDs that cisgender individuals avoid are actively sought by trans masculine individuals for gender-affirming care. Could this be an important lens for understanding PIED use?
Agree 100% that those androgenic affects are what some people are after. I think we have a long history of viewing these drugs through a hegemonic lens (with many researchers having touched on this both in and outside Australia). I think this is a super important space. As a few people from community have said, and I agree with, there are no ‘side’ effects… there are just ‘effects’, and the way the person uses the drug and the underlying motivations of that usage will dictate which are ‘wanted/intended’ and which are not.
It has been reported that methadone (used in opioid maintenance therapy or OMT) can reduce testosterone levels. Are there any known cases of individuals self-managing their testosterone or hormone levels instead of seeking GP management?
This is interesting! Have come across people who are recently off the program and using testosterone (for various reasons), but not concurrently yet. Will keep an eye out in this space.
Can bacteriostatic water be substituted with sterile water for injections?
No, Bacteriostatic water shouldn’t be interchangeable – sterile water is single use, bacstat water contains benzyl alcohol (usually) which is important for vials which are multi-use (e.g., peptides).
What needle length and gauge should be used for steroid/PIED injections?
Check out this Hi-Ground Resource that includes a table detailing the needle length and gauge that should be used for steroid/PIED injections.
Do people who use PIEDS identify with the term PIEDS?
Usually steroids or PEDs (performance enhancing drugs) works fine as a ‘professional’ term.
Where do SARMs fit into the broader PIEDs category?
SARMs => Selective Androgen Receptor Modulators, designed to be ‘safer’ alternatives to more ‘traditional’ androgens (e.g., nandrolone). They are taken orally (as a capsule/pill usually) and offer up people similar (but reportedly much milder) effects (e.g., muscle growth, strength etc.). We actually still do not know the longer-term effects on peoples’ health.
Do oil-based steroids flow easily through finer needles?
If it is a thicker oil the flow will be slower and that is totally fine. For e.g., you can backload a g27 with a thick oil (e.g., 0.3mil) if wanting to do small amount of injections daily. That could then go into, for e.g., rear deltoid/lateral tricep. Just need to accept ‘flow’ will be slow, so may be ‘pushing’ it through for a little while (and be patient with this).
As a GP interested in harm minimisation but with limited experience in PIEDs, who should I refer patients to for further support?
Happy to consult via email (t.piatkowski@griffith.edu.au) and look at ways we can support people together through health monitoring if you would like. Can also link you in with other medical professionals in this field who specialise (e.g., Dr Thomas O’Connor).
How do we, as peers who use illicit drugs, talk about harm reduction in ways that connect with PIED users?
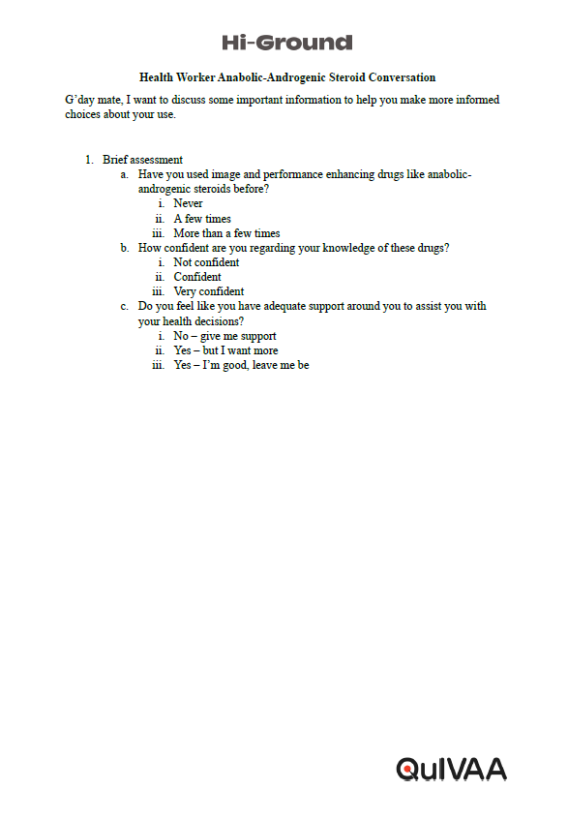
No one is expecting you to be an expert in PIEDs. What matters is engaging positively and accepting that some people are comfortable and well-informed about their use – while others are not and that is probably where more of the knowledge sharing can come in. In each instance, you have something valuable to offer— the provision of equipment and/or services. As discussed in the webinar, focusing on straightforward harm reduction practices like safe injecting to prevent bacterial infections, sanitary vial storage, and site rotation can be a good starting point, rather than focusing on blood-borne virus transmission initially.
Do performance-enhancing drug (PIED) users look down on people who inject illicit drugs?
My research indicates that some ‘othering’ can occur between people who use PIEDs and people who inject other illicit drugs (e.g., meth), with a common perception that PIEDs are ‘enhancing,’ while other substances are viewed as more ‘destructive’. However, this view is person-specific, and many people actually do hold a more inclusive perspective.
Is there any evidence or guidance on the use of steroids to help alleviate symptoms associated with menopause?
Research indicates that testosterone may enhance libido, particularly for women experiencing peri/menopause. A 2023 review in a pharmaceutical journal confirmed that there are testosterone treatments available specifically for women, which can help increase sex drive during this transitional phase. Research has shown that adding testosterone to hormonal therapy can improve sexual function and overall well-being in menopausal women, enhancing aspects like desire, pleasure, arousal, orgasm, and self-image.
Beyond boosting libido, testosterone can also alleviate urogenital, psychological, and physical symptoms, improve bone density, and enhance cognitive performance when used alongside estrogen in hormone replacement therapy. Many women report increased mood, focus, motivation, and energy levels with testosterone (Scott & Newson, 2020).
Given that women naturally produce testosterone, which decreases during menopause, there is a need for further research to ensure women can access effective treatment. Before considering the use of testosterone it is essential to consult a hormone specialist/trusted GP before making any decisions about how to manage personal peri/menopausal symptoms.
What are the healthcare barriers women face when accessing steroids?
From personal experience, the GPs I consulted were reluctant to discuss my personal use of steroids. I received no harm reduction advice, only an abstinence framework. It took considerable effort and self-advocacy to have my hormones tested by a female doctor, who eventually agreed to order bloodwork to assess my hormonal levels.
My experiences within the healthcare system align with the observations made by Cox, Piatkowski, and McVeigh (2024), an article highlighting that stigma and a lack of confidence in understanding steroids and related substances can create barriers to accessing support regarding steroid use, information, and harm reduction discussions, particularly for women and their choices around steroid use.
Research and my experience indicate that the lack of knowledge and confidence within the healthcare system is a significant barrier for women seeking support with regards to their use of steroids.
