
वेबिनार: प्रदर्शन और छवि बढ़ाने वाली दवाओं का उपयोग करने वाले लोगों को समझना और उनका जवाब देना
प्रदर्शन और छवि बढ़ाने वाली दवाएं (पीआईईडी) सबसे तेजी से बढ़ती दवा श्रेणी है, जो पूरे ऑस्ट्रेलिया में एनएसपी आंकड़ों में दिखाई देती है।
स्टेरॉयड और अन्य प्रदर्शन एवं छवि बढ़ाने वाली दवाओं (पीआईईडीएस) का उपयोग करने वाले व्यक्तियों की संख्या बढ़ती जा रही है, जो इंजेक्शन लगाने के उपकरण के लिए सुई और सिरिंज कार्यक्रमों का उपयोग कर रहे हैं।
पीआईईडी के बारे में अधिक जानने तथा उनका उपयोग करने वालों को प्रभावी ढंग से सहायता प्रदान करने के तरीके के बारे में जानने के लिए यह ऑनलाइन प्रशिक्षण वेबिनार देखें।

डॉ. टिम पियाटकोव्स्की
ग्रिफ़िथ विश्वविद्यालय और QuIVAA
डॉ. टिम निम्नलिखित विषयों पर चर्चा करेंगे: पीआईईडी को परिभाषित करना, यह समझना कि पीआईईडी का उपयोग कौन और क्यों करता है, लोग पीआईईडी का उपयोग किस प्रकार करते हैं, पीआईईडी के उपयोग के लिए उपयुक्त उपकरणों की सिफारिश करना, तथा हानि न्यूनीकरण संबंधी जानकारी प्रदान करना।

सोन्या वेइथ
क्यूआईवा
सोनिया महिलाओं और PIED के उपयोग पर चर्चा करेंगी।
क्यूआईवा/हाई-ग्राउंड प्रशिक्षण में संदर्भित संसाधन
लाइव प्रशिक्षण के दौरान पूछे गए प्रश्नों के उत्तर डॉ. टिम और सोन्या ने दिए
उपयोगकर्ता स्टेरॉयड का परीक्षण कहां करा सकते हैं? (ऑस्ट्रेलिया के आसपास विशिष्ट स्थानों पर?)
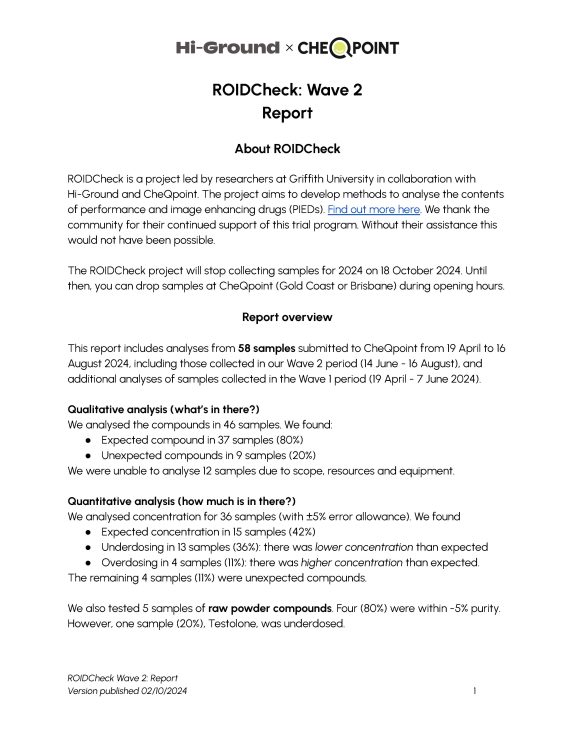
चेकपॉइंट ब्रिसबेन और गोल्ड कोस्ट में हमारे द्वारा चलाए जा रहे वर्तमान स्टेरॉयड जाँच परीक्षण के लिए संग्रह स्थल रहे हैं। अंतिम ड्रॉप-ऑफ 18 थेवां हमारे वेव 3 विश्लेषण के लिए अक्टूबर 2024।
अब तक की तरंगों के परिणाम यहां देखें – स्टेरॉयड जाँच परियोजना के परिणाम! – hi-ground.org
2025 तक इस स्थान पर नजर रखें।
पीआईईडी के कई दुष्प्रभाव जिनसे सिजेंडर व्यक्ति बचते हैं, उन्हें ट्रांस मैस्कुलिन व्यक्ति लिंग-पुष्टि देखभाल के लिए सक्रिय रूप से चाहते हैं। क्या यह पीआईईडी के उपयोग को समझने के लिए एक महत्वपूर्ण लेंस हो सकता है?
इस बात से सहमत हूं कि एंड्रोजेनिक को प्रभावित करता है कुछ लोग इसी के पीछे हैं। मुझे लगता है कि हम इन दवाओं को एक आधिपत्यवादी नजरिए से देखने का एक लंबा इतिहास रहा है (ऑस्ट्रेलिया और उसके बाहर कई शोधकर्ताओं ने इस पर विचार किया है)। मुझे लगता है यह एक बहुत ही महत्वपूर्ण स्थान है। जैसा कि समुदाय के कुछ लोगों ने कहा है, और मैं इससे सहमत हूँ, इसका कोई 'दुष्प्रभाव' नहीं है... बस 'प्रभाव' हैं', और जिस तरह से व्यक्ति इसका उपयोग करता है दवाई और उस प्रयोग के अंतर्निहित उद्देश्य यह निर्धारित करेंगे कि कौन सी बातें 'वांछित/इरादाबद्ध' हैं और कौन सी नहीं।
यह बताया गया है कि मेथाडोन (ओपिओइड रखरखाव चिकित्सा या OMT में उपयोग किया जाता है) टेस्टोस्टेरोन के स्तर को कम कर सकता है। क्या ऐसे कोई ज्ञात मामले हैं जिनमें व्यक्ति GP प्रबंधन की तलाश करने के बजाय अपने टेस्टोस्टेरोन या हार्मोन के स्तर को स्वयं प्रबंधित करता है?
यह दिलचस्प है! पास होना ऐसे लोगों से मिलें जो हाल ही में कार्यक्रम से बाहर निकलना और टेस्टोस्टेरोन का उपयोग करना (के लिए कई कारण), लेकिन अभी तक समवर्ती नहीं। इस क्षेत्र पर नज़र रखूँगा।
क्या इंजेक्शन के लिए जीवाणुरहित जल को जीवाणुरहित जल से प्रतिस्थापित किया जा सकता है?
नहीं, जीवाणु-स्थैतिक जल नहीं करना चाहिए विनिमेय हो – बाँझ पानी है एक बार इस्तेमाल लायक, बैकस्टैट पानी रोकना बेंज़िल अलकोहोल (आमतौर पर) जो बहुउपयोगी शीशियों (जैसे, पेप्टाइड्स) के लिए महत्वपूर्ण है।
स्टेरॉयड/पीआईईडी इंजेक्शन के लिए किस लंबाई और गेज की सुई का उपयोग किया जाना चाहिए?
इस हाई-ग्राउंड संसाधन को देखें जिसमें स्टेरॉयड/पीआईईडी इंजेक्शन के लिए उपयोग की जाने वाली सुई की लंबाई और गेज का विवरण देने वाली तालिका शामिल है।
क्या PIEDS का प्रयोग करने वाले लोग PIEDS शब्द से परिचित हैं?
आमतौर पर स्टेरॉयड या पीईडी (प्रदर्शन बढ़ाने वाली दवाएं) एक 'पेशेवर' शब्द के रूप में ठीक काम करता है।
SARMs व्यापक PIEDs श्रेणी में कहां फिट होते हैं?
SARMs => चयनात्मक एण्ड्रोजन रिसेप्टर मॉड्यूलेटर, 'सुरक्षित' विकल्प के रूप में डिजाइन किए गएअधिक 'पारंपरिक' एण्ड्रोजन (जैसे, नैंड्रोलोन) की ओर रुख करते हैं। इन्हें मौखिक रूप से लिया जाता है (आमतौर पर कैप्सूल/गोली के रूप में) और लोग समान (लेकिन कथित तौर पर बहुत हल्के) प्रभाव (जैसे, मांसपेशियों की वृद्धि, ताकत आदि)। हम वास्तव में अभी भी नहीं जानते दीर्घकालीन लोगों के स्वास्थ्य पर प्रभाव.
क्या तेल आधारित स्टेरॉयड महीन सुइयों के माध्यम से आसानी से प्रवाहित होते हैं?
यदि तेल गाढ़ा होगा तो प्रवाह धीमा होगा और यह बिलकुल ठीक। के लिए उदाहरण के लिए, आप एक मोटी तेल के साथ एक g27 backload कर सकते हैं (उदाहरण के लिए, 0.3 मिलियन) यदि आप करना चाहते हैं छोटा मात्रा प्रतिदिन इंजेक्शन की संख्या। फिर यह उदाहरण के लिए, रियर डेल्टोइड/लेटरल में जा सकता है ट्राइसेपबस 'प्रवाह' को स्वीकार करने की आवश्यकता है, इसलिए यह धीमा होगा शायद इसे थोड़ी देर तक 'धकेलते' रहें (और इसमें धैर्य रखें)।
एक GP के रूप में, जो हानि न्यूनीकरण में रुचि रखता है, लेकिन PIEDs में सीमित अनुभव के साथ, मुझे आगे की सहायता के लिए रोगियों को किसके पास भेजना चाहिए?
ईमेल के माध्यम से परामर्श करने में खुशी होगी (t.piatkowski@griffith.edu.au) और अगर आप चाहें तो स्वास्थ्य निगरानी के ज़रिए हम लोगों को एक साथ कैसे सहयोग कर सकते हैं, इस पर भी नज़र डाल सकते हैं। हम आपको इस क्षेत्र के अन्य चिकित्सा पेशेवरों से भी जोड़ सकते हैं जो विशेषज्ञ (उदाहरणार्थ, डॉ. थॉमस ओ'कॉनर)।
हम, अवैध दवाओं का उपयोग करने वाले साथियों के रूप में, PIED उपयोगकर्ताओं के साथ जुड़ने के तरीकों से हानि न्यूनीकरण के बारे में कैसे बात करते हैं?
कोई भी आपसे यह उम्मीद नहीं कर रहा है कि आप PIEDs में विशेषज्ञ। जो बात मायने रखती है वह है सकारात्मक रूप से जुड़ना और यह स्वीकार करना कि कुछ लोग उनके उपयोग के बारे में सहज और अच्छी तरह से सूचित हैं - जबकि अन्य नहीं हैं और शायद यहीं पर अधिक ज्ञान साझा किया जा सकता है। प्रत्येक उदाहरण में, आपके पास देने के लिए कुछ मूल्यवान है - उपकरण और/या सेवाओं का प्रावधान। जैसा कि चर्चा की गई है वेबिनारजीवाणु संक्रमण को रोकने के लिए सुरक्षित इंजेक्शन लगाने, सैनिटरी शीशी भंडारण और साइट रोटेशन जैसे सीधे नुकसान कम करने वाले तरीकों पर ध्यान केंद्रित करना एक अच्छा प्रारंभिक बिंदु हो सकता है, बजाय इसके कि इस पर ध्यान केंद्रित किया जाए। रक्त जनित वाइरस प्रसारण शुरू में।
क्या प्रदर्शन-वर्धक दवा (पीआईईडी) के उपयोगकर्ता उन लोगों को नीची नजर से देखते हैं जो अवैध दवाओं का इंजेक्शन लेते हैं?
मेरा शोध इंगित करता है पीआईईडी का उपयोग करने वाले लोगों और अन्य अवैध दवाओं (जैसे, मेथ) को इंजेक्ट करने वाले लोगों के बीच कुछ 'अन्यकरण' हो सकता है, जिसमें एक आम बात है धारणा पीआईईडी 'बढ़ाने वाले' हैं, जबकि अन्य पदार्थों को अधिक 'विनाशकारी' माना जाता है'. हालाँकि, यह दृष्टिकोण व्यक्ति-विशिष्ट है, और कई लोग वास्तव में अधिक समावेशी दृष्टिकोण रखते हैं।
क्या रजोनिवृत्ति से जुड़े लक्षणों को कम करने में स्टेरॉयड के उपयोग पर कोई सबूत या मार्गदर्शन उपलब्ध है?
शोध से पता चलता है कि टेस्टोस्टेरोन कामेच्छा को बढ़ा सकता है, खासकर पेरी/मेनोपॉज का अनुभव करने वाली महिलाओं के लिए। एक फार्मास्युटिकल जर्नल में 2023 की समीक्षा ने पुष्टि की कि महिलाओं के लिए विशेष रूप से टेस्टोस्टेरोन उपचार उपलब्ध हैं, जो इस संक्रमणकालीन चरण के दौरान सेक्स ड्राइव को बढ़ाने में मदद कर सकते हैं। शोध से पता चला है कि हार्मोनल थेरेपी में टेस्टोस्टेरोन को शामिल करने से रजोनिवृत्त महिलाओं में यौन क्रिया और समग्र कल्याण में सुधार हो सकता है, जिससे इच्छा, आनंद, उत्तेजना, संभोग और आत्म-छवि जैसे पहलुओं में वृद्धि हो सकती है।
कामेच्छा को बढ़ाने के अलावा, टेस्टोस्टेरोन मूत्रजननांगी, मनोवैज्ञानिक और शारीरिक लक्षणों को भी कम कर सकता है, हड्डियों के घनत्व में सुधार कर सकता है और हार्मोन रिप्लेसमेंट थेरेपी में एस्ट्रोजन के साथ उपयोग किए जाने पर संज्ञानात्मक प्रदर्शन को बढ़ा सकता है। कई महिलाएं टेस्टोस्टेरोन के साथ मूड, फोकस, प्रेरणा और ऊर्जा के स्तर में वृद्धि की रिपोर्ट करती हैं (स्कॉट और न्यूसन, 2020)।
यह देखते हुए कि महिलाएं स्वाभाविक रूप से टेस्टोस्टेरोन का उत्पादन करती हैं, जो रजोनिवृत्ति के दौरान कम हो जाता है, यह सुनिश्चित करने के लिए आगे के शोध की आवश्यकता है कि महिलाएं प्रभावी उपचार तक पहुँच सकें। टेस्टोस्टेरोन के उपयोग पर विचार करने से पहले व्यक्तिगत पेरी/मेनोपॉज़ल लक्षणों को प्रबंधित करने के तरीके के बारे में कोई भी निर्णय लेने से पहले हार्मोन विशेषज्ञ/विश्वसनीय जीपी से परामर्श करना आवश्यक है।
स्टेरॉयड प्राप्त करने में महिलाओं को किन स्वास्थ्य संबंधी बाधाओं का सामना करना पड़ता है?
व्यक्तिगत अनुभव से, मैंने जिन GPs से परामर्श किया, वे स्टेरॉयड के मेरे व्यक्तिगत उपयोग पर चर्चा करने के लिए अनिच्छुक थे। मुझे कोई नुकसान कम करने की सलाह नहीं मिली, केवल संयम की रूपरेखा दी गई। एक महिला डॉक्टर द्वारा मेरे हार्मोन की जांच करवाने के लिए मुझे काफी प्रयास और आत्म-वकालत करनी पड़ी, जो अंततः मेरे हार्मोनल स्तरों का आकलन करने के लिए रक्त परीक्षण का आदेश देने के लिए सहमत हो गई।
स्वास्थ्य सेवा प्रणाली के भीतर मेरे अनुभव कॉक्स, पियाटकोव्स्की और मैकवे (2024) द्वारा किए गए अवलोकनों के अनुरूप हैं, एक लेख जिसमें बताया गया है कि स्टेरॉयड और संबंधित पदार्थों को समझने में कलंक और आत्मविश्वास की कमी स्टेरॉयड के उपयोग, सूचना और हानि में कमी की चर्चाओं के संबंध में समर्थन प्राप्त करने में बाधाएं पैदा कर सकती है, विशेष रूप से महिलाओं और स्टेरॉयड के उपयोग के बारे में उनके विकल्पों के लिए।
शोध और मेरे अनुभव से पता चलता है कि स्वास्थ्य सेवा प्रणाली में ज्ञान और आत्मविश्वास की कमी, स्टेरॉयड के उपयोग के संबंध में सहायता चाहने वाली महिलाओं के लिए एक महत्वपूर्ण बाधा है।
